It has been over 80 years since Coons et al. first reported the use of immunohistochemistry (IHC) to visualize pneumococcal bacteria in infected tissue samples. During that time, the underlying principles of IHC have remained the same, meaning modern day researchers may suffer similar pitfalls to their predecessors. Here, we look at four common IHC mistakes and suggest how these may be avoided.
Frozen and FFPE tissue are not one and the same
According to Katie Crosby, Sr. Director for Antibody Applications and Validation at Cell Signaling Technology, tissue samples are commonly categorized as formalin-fixed paraffin-embedded (FFPE), perfused cryosections (fixed-frozen), or fresh frozen. Because the preservation method can influence how antibody reagents will perform, it is unreasonable to assume that an antibody will work across all sample types.
Search IHC kits Search Now Search our directory to find IHC kits for your research needs.
“Before being incubated with primary antibodies, tissue samples must undergo multiple processing steps in accordance with the preservation method used,” she explains. “Each of these steps can affect antigens differently, which ultimately impacts antibody functionality. For this reason, sample type is one of the most important factors to consider when selecting antibodies for IHC. Researchers should ensure that the antibody of interest has been shown to work with samples prepared in the same fashion as those they intend to test.”
Epitope retrieval may be required
Epitope retrieval is frequently recommended when working with FFPE tissues, and may also be necessary on frozen sections that have been fixed with aldehyde-based reagents like formalin. To avoid compromising target detection, epitope retrieval should always be carefully tailored to the system in question.
“Individual experimental conditions, such as the fixation method and duration, type of tissue, target antigen, and chosen antibody, will all determine whether there is a need for epitope retrieval,” reports Emily Cartwright, Senior Product Marketing Specialist, Antibodies at Bio-Techne. “Generally, heat-induced epitope retrieval (HIER) is preferred over proteolytic-induced epitope retrieval (PIER), which is harsher on tissue and best saved for heavily cross-linked samples. When establishing your protocol, epitope retrieval conditions may need to be optimized.”
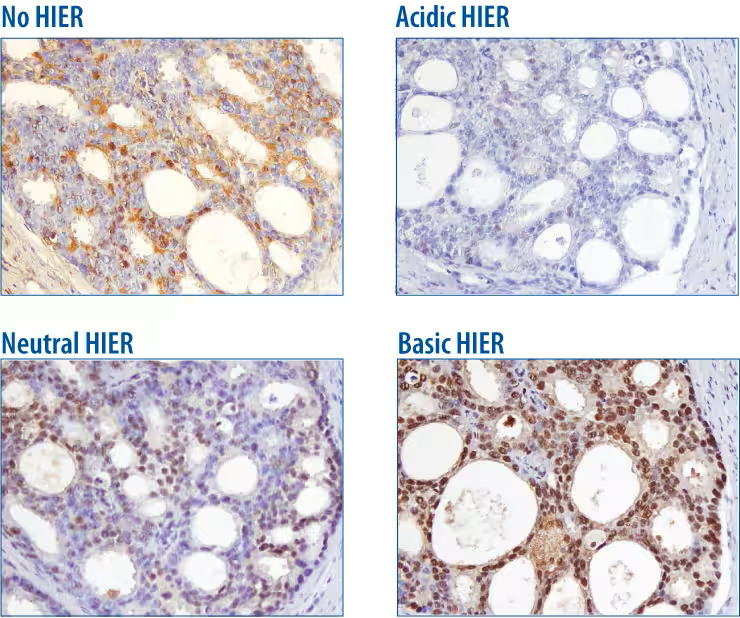
Antigen retrieval improves IHC detection of p27. p27 was detected in paraffin-embedded human prostate cancer sections following incubation of tissue for 10 minutes at 95 °C in the specified antigen retrieval solution. Compared to no HIER treatment, p27 detection was enhanced following incubation in neutral (pH 7.0) and basic (pH 9.5) HIER solution but not the acidic (pH 5.0) HIER solution. p27 was detected using Rat Anti-Human/Mouse/Rat p27/Kip1 Monoclonal Antibody (brown). Images provided by Bio-Techne.
“To optimize epitope retrieval, I recommend starting with a high-expression tissue,” says Rachel Gonzalez, Senior Scientist, Antibody Research and Development at OriGene Technologies. “That way, you can determine whether the antibody is going to work in IHC without having to use multiple titers. For example, if I am testing PDL1 or EGFR antibodies, I use placental tissue, or if I am testing Ki67 antibodies, I use tonsil tissue. For proteins where finding high-expression tissue is difficult, cDNA-generated CytoSections are a good option. These serve as positive/negative controls where target expression is confirmed for accuracy and specificity by an immunoassay.”
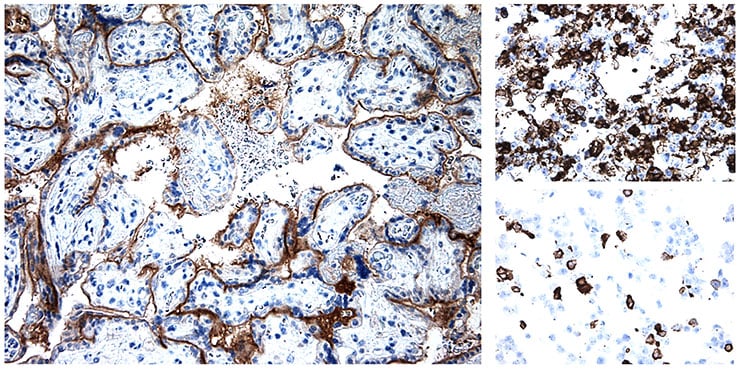
IHC staining with a PD-L1 antibody. Left panel: placenta; top right panel: CytoSection TS413071P5 (transient over-expression of PD-L1 NM_014143 in HEK293T cells); bottom right panel: CytoSection TS431972P5 (transient over-expression of PD-L1 NM_001267706 in HEK293T cells). Image provided by OriGene Technologies.
Additional blocking steps are often necessary
While most researchers are aware of the need to block non-specific antibody binding with reagents such as normal serum or bovine serum albumin (BSA), IHC often requires additional blocking steps. Erika Leonard, Director of R&D at Vector Laboratories, explains that these include blocking for endogenous enzyme activity. “IHC detection often involves using secondary antibodies conjugated to reporter enzymes, such as horseradish peroxidase and alkaline phosphatase, that convert chromogenic substrates into colored precipitates,” she says. “Some tissues have high endogenous peroxidase (e.g., blood-heavy tissues such as the spleen and kidney) and phosphatase (e.g., kidney, intestine, and liver), which can metabolize chromogenic substrates to cause high background. These effects can be mitigated with a reagent such as BLOXALL™ Endogenous Peroxidase and Alkaline Phosphatase Blocking Solution, which inactivates endogenous peroxidase, pseudoperoxidase, and alkaline phosphatase in FFPE tissue sections, frozen tissue sections, and cell preparations.”
If you are using a detection system based on the high-affinity interaction between biotin and avidin/streptavidin, you may also need to block endogenous biotin. “A biotin block is especially useful for tissues that express high levels of biotin, such as kidney and liver,” notes Crosby. “Alternatively, there are now highly sensitive polymer-based detection reagents available that eliminate the need for biotin blocking, like SignalStain® Boost IHC Detection Reagent (HRP, Rabbit) that is used to detect rabbit primary antibodies with HRP-based substrates.”
Another type of block worth considering is mouse-on-mouse blocking, which prevents anti-mouse secondary antibodies from binding to endogenous IgG in mouse tissues. Although this problem can be circumvented by using a primary antibody raised in a different host species from the sample material, such an antibody may not always be available. “At OriGene, we perform mouse-on-mouse blocking not only on mouse tissues but also when doing sequential staining of multiple mouse primaries on human tissue,” says Gonzalez. “In addition, we include a rabbit-on-rabbit block in our multi-staining kits and offer Klear Human Kits for screening human primary antibodies on human tissue.”
Finally, you will want to think about blocking autofluorescence if using immunofluorescent detection. “Autofluorescence occurs when molecules other than the antigen-bound antibody complex emit a fluorescent signal,” says Leonard. “There are many tissue components that can autofluoresce, including the heme groups of red blood cells, as well as collagen, elastin, NADH, and lipofuscin. The fixation process can also contribute to autofluorescence as formalin-induced cross-links can emit fluorescence in a broad range of wavelengths. One way of addressing this is to use the Vector® TrueVIEW™ Autofluorescence Quenching Kit, which diminishes autofluorescence from non-lipofuscin sources to improve the signal-to-noise ratio.”
Antibodies are often not to blame for weak staining
When weak IHC staining is observed, researchers often blame primary antibodies. But there are other potential causes for weak staining, many of which can be found in our IHC Troubleshooting Guide. “Provided your antibody is validated for the IHC application and suitable for use with your chosen species, there are several steps you can take to improve your staining,” comments Cartwright. “These include titrating the antibody to make sure it is at saturating concentration for your experiment, as well as testing different incubation times. Additionally, crosslinks due to fixation can impede antibody binding, so an epitope retrieval step may be needed. If you are using a new lot of an antibody, I recommend testing it against the previous lot to verify performance.”