When immunohistochemistry (IHC) was first developed, it allowed researchers to detect a single biomarker per slide. Today, it is possible to simultaneously visualize many different targets—saving both time and precious sample material in the process. This article summarizes the main methods for traditional IHC before delving into the advantages of multiplexing. It also highlights some of the available multiplex IHC technologies and describes an established approach to deal with the vast quantities of data that multiplex IHC generates.
Traditional IHC methods
IHC was first conceptualized in 1930, but it was not until 1941 that Coons et al. reported the use of a FITC-labeled antibody to visualize antigens in tissue sections.1,2 Horseradish peroxidase (HRP) antibody labels were introduced in 1966, followed by colloidal gold labels in 1971 and alkaline phosphatase (AP) labels in 1978.3-5 At around the same time, methods to increase sensitivity were developed, including Peroxidase/Anti-Peroxidase (PAP) detection, Avidin-Biotin Complex (ABC) detection, and Labeled Streptavidin Biotin (LSAB) detection. Subsequently, polymer-based detection methods evolved to further boost sensitivity and eliminate the potential for false positive staining due to endogenous biotin. All of these techniques are still in use today.
Search IHC kits Search Now Search our directory to find IHC kits for your research needs.
“Factors influencing method selection include target abundance, spatial distribution, and workflow constraints,” says Erika Leonard, Director of R&D at Vector Laboratories. “When antigens are closely co-localized, fluorescence is often preferred because the small size of fluorophore labels enables precise visualization of multiple targets within the same cellular compartment. Instrumentation is also critical: advanced fluorescence microscopy, multispectral imaging, and automation platforms support higher-plex fluorescent workflows, whereas brightfield systems more commonly align with chromogenic approaches. Tissue properties such as autofluorescence, along with sensitivity and dynamic range requirements, are further considerations.”
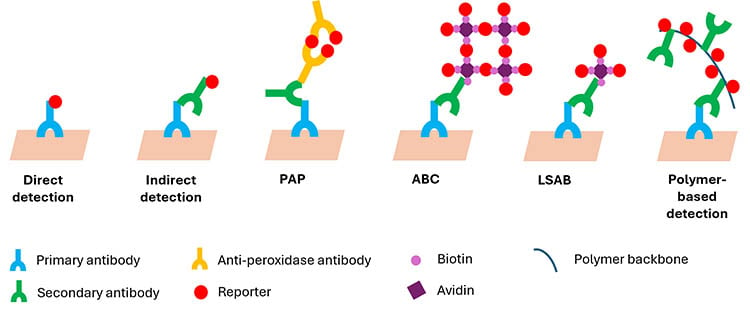
Traditional IHC methods. Direct detection involves the fewest protocol steps, but indirect detection, Peroxidase/Anti-Peroxidase (PAP) detection, Avidin-Biotin Complex (ABC) detection, Labeled Streptavidin Biotin (LSAB) detection, and polymer-based detection all provide signal amplification by increasing the number of reporter molecules that are localized to the target site. PAP, ABC, and LSAB use a peroxidase reporter, whereas direct detection, indirect detection, and polymer-based detection can alternatively use alkaline phosphatase or a fluorescent dye.
Advantages of multiplex IHC
According to Paulina Leung-Lee, Senior Marketing Portfolio Manager for Scaling Biology at Cell Signaling Technology (CST), traditional singleplex IHC is a robust but inherently reductionist method, limited to one marker per slide, semi-quantitative scoring, and heavy tissue consumption. “In contrast, multiplex IHC is a high dimensional, spatially resolved approach that can measure many markers simultaneously on a single section, quantify co-expression and cell–cell interactions in situ, and more effectively handle tumor heterogeneity and scarce samples through maximal information per section and reduced sampling bias,” she says. “This enables sophisticated analytics, improved predictive power for complex biological responses, and deeper mechanistic insight in translational research.”
Importantly, multiplex IHC has value throughout the entire drug development workflow. “In a pre-clinical space, you have the luxury of tissue, such as from a xenograft or other tissue from in vivo models,” notes Elizabeth Ross, Director of Scientific Business Development at CellCarta. “This allows you to ask broad questions of your samples, like defining a drug’s mechanism of action, characterizing the complex microenvironment of effector cell populations, or tracking the resolution of pathology. In the diagnostic or clinical setting, patient tissue is limited and precious. Here, multiplex IHC allows for the collection of as much information as possible from a minimum of slides. Furthermore, cell phenotypes can indicate cell function when the multiplex panel contains markers of cell activation, suppression, division, antigen presentation, necrosis, and apoptosis.”
Advanced multiplex IHC technologies
While multiplex IHC technologies differ considerably in terms of how they work, all are relatively easy to use. The following are three leading examples:
Vector Laboratories’ VectaPlex™ Antibody Removal Kit efficiently removes antibodies and other non-covalently bound detection reagents from FFPE tissue sections via a simple room-temperature protocol. It is compatible with immunofluorescence, fluorescent tyramide, and chromogenic immunohistochemistry workflows—both manual and automated. By preserving tissue morphology across multiple staining cycles, even in delicate tissues such as breast and skin, VectaPlex maintains antigen integrity and eliminates the complexity of optimizing primary antibody concentrations based on staining order.
A composite image of FFPE stomach generated from six rounds of immunofluorescence staining using VectaPlex. Mouse primary antibodies for CD20 (red), CD34 (yellow), Desmin (cyan), AE1/AE3 (magenta), CD3 (gray), and Vimentin (green) were detected with DyLight™ 488 horse anti-mouse IgG. Blue indicates DAPI stain. Background fluorescence was suppressed using Vector® TrueView® Autofluorescence Quencher Kit.
SignalStar® Multiplex IHC from CST uses high-throughput, mid-plex IHC assays to label up to 8 targets in FFPE tissues simultaneously with flexible, highly validated antibody panels, configurable using the SignalStar Multiplex IHC Panel Builder. The technology uses a combination of oligonucleotides and fluorophores to amplify the antibody signal, allowing for the detection of targets with low expression levels, such as FoxP3. Because SignalStar antibodies and fluorophores are interchangeable, researchers can redesign panels with minimal optimization. SignalStar technology is up to 70% faster from sample to imaging than other traditional mIHC methods and can be run on an automated slide stainer, reducing up to 12 hours hands-on time and minimizing human error.

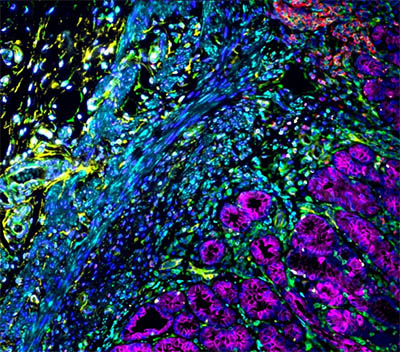
SignalStar immunohistochemical analysis of paraffin-embedded human squamous cell lung carcinoma using Pan-Keratin (C11) & CO-0003-488 SignalStar Oligo-Antibody Pair #63566 (cyan), CD68 (D4B9C) & CO-0007-594 SignalStar Oligo-Antibody Pair #77318 (orange), SIRPα/SHPS1 (D6I3M) & CO-0034-647 SignalStar Oligo-Antibody Pair #80150 (pink), CD163 (D6U1J) & CO-0022-750 SignalStar Oligo-Antibody Pair #71043 (magenta), CD206/MRC1 (E2L9N) & CO-0035-488 SignalStar Oligo-Antibody Pair #99626 (green), CD11c (D3V1E) & CO-0017-594 SignalStar Oligo-Antibody Pair #85384 (yellow), CD45 (Intracellular Domain) (D9M8I) & CO-0013-647 SignalStar Oligo-Antibody Pair #32740 (red), and HLA-DRA (E9R2Q) & CO-0023-750 SignalStar Oligo-Antibody Pair #58446 (white). All fluorophores have been assigned a pseudocolor, as indicated. Multiplex staining was performed on the BOND RX Fully Automated Research Stainer by Leica Biosystems.
The COMET™ Multiplex Immunofluorescence workflow used by CellCarta is based on sequential immunofluorescence (seqIF™) with pairs of unlabeled primary antibodies and matched Cy5- and TRITC-labeled secondary antibodies, with DAPI as a nuclear stain. Samples are processed through up to 20 automated staining cycles, each of which produces a stitched and stacked image that can be analyzed using the Lunaphore HORIZON™ software or exported for downstream analysis using other software. Lunaphore technology allows for multiplex panels to be constructed with either protocol-optimized SPYRE® antibodies or unconjugated primary antibodies. Panel validation at CellCarta requires that each target is cross-validated with chromogenic single or low-plex stained tissue. Compared to traditional IHC, which can take 20 hours for sequential staining, scanning, and analysis of 4 targets, the COMET multiplex immunofluorescence workflow can detect 20 targets within the same timeframe.
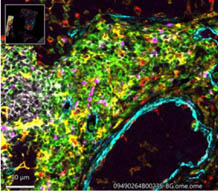
A composite image of a multi-tissue block containing one tonsil and two breast cancer tissues was stained and scanned on the Lunaphore COMET instrument using primary mouse and rabbit SPYRE™ antibodies from the Lunaphore Immuno-Oncology Core Panel. Sequential staining, scanning and elution rounds were performed using a blue DAPI nuclear stain, unlabeled primary mouse and rabbit antibodies followed by anti-isotype secondary antibodies labeled with AlexaFluor® 555 or AlexaFluor® 647. Images from stain and scan cycles containing isotype controls and fluorophore labeled secondary antibodies were used to subtract background fluorescence before image analysis. Channel labels are: CD3 (green), FOXP3 (purple), CD20 (white), CD11c (yellow), CD68 (red), and aSMA (light blue). The image shows one of the two breast cancer tissues.
Challenges for data handling
A major challenge for multiplex IHC is the size of the images and the interpretation of the huge quantities of data that are produced. “At CellCarta, we have had to develop an effective strategy for image management and analysis,” says Ross. “A typical chromogenic, singleplex image is between 1 and 2 gigabytes. With COMET, three whole slide images are captured per cycle and, depending upon the size of the panel, the final raw image file can be 200 to 300 gigabytes. Before analysis, background is subtracted using the Lunaphore HORIZON™ software, which reduces the file size by 40–50%. We then move the image into our standard cloud-based analysis workflow using Halo AI or Halo Link to obtain object data like stained cell numbers and densities. With this approach, the image is analyzed once and the resulting object data files can be queried and re-queried for phenotypic and spatial relationships as the scientific insight evolves.”
Conclusion
While traditional IHC remains popular with researchers, the use of multiplex IHC is on the rise—driven by the growing availability of user-friendly technologies. “Through simultaneous spatial analysis of multiple biomarkers within a single tissue section, multiplex IHC enhances experimental efficiency and can reveal cellular interactions, co-localization, and microenvironmental context that are difficult to resolve using serial sections,” says Leonard. “For these reasons, multiplex IHC is increasingly critical in oncology, immunology, and translational research, where complex signaling networks and tissue heterogeneity must be understood in spatial context.”
References
1. Reiner L. On the chemical alteration of purified antibody-proteins. Science. 1930;72(1871):483-484.
2. Coons, A. H., Creech, H. J. and Jones, R. N. Immunological properties of an antibody containing a fluorescent group. Proc. Soc. Expt. Biol. Med. 1941;47(2):200-202
3. Nakane PK and Pierce GB Jr. Enzyme-labeled antibodies: preparation and application for the localization of antigens. J Histochem Cytochem. 1966;14(12):929-931.
4. Faulk WP, Taylor GM. An immunocolloid method for the electron microscope. Immunochemistry. 1971;8(11):1081-1083
5. Mason DY, Sammons R. Alkaline phosphatase and peroxidase for double immunoenzymatic labelling of cellular constituents. J Clin Pathol. 1978;31(5):454-460.