A main advantage of IHC over other immunodetection techniques is that it provides spatial context to antigen expression. With IHC, researchers can see where within a tissue a particular protein is localized and can determine its relative expression between different cell types. Although modern IHC benefits from a more streamlined workflow and higher plex compared to early forms of the technique, care is still required to ensure IHC data is accurate. In this article, we comment on how IHC has evolved and suggest some strategies to achieve successful staining.
IHC is widely applicable
According to Hartmut Pohl, Ph.D., application scientist at Enzo Life Sciences, IHC has utility wherever visualizing tissue anatomy is critical. “Unlike other commonly used immunodetection methods, IHC provides spatial and morphological information alongside immunostaining,” he says. “This allows histo-anatomical and histo-pathological analyses in combination with superimposed specific marker staining to identify cells or their status within a chosen tissue.” In turn, these features of IHC mean it is applicable to a broad range of studies—spanning basic research all the way through to clinical diagnostics—and make it the method of choice when the composition, cellular characteristics, and structure of native tissues must be preserved.
Search IHC kits Search Now Search our directory to find the right IHC kit for your research needs.
“Even scarce cell types in a tissue can be identified using IHC,” comments Abel Zhang, R&D leader at Proteintech. “For example, staining of CD3 or CD8 can identify tumor-infiltrating lymphocytes.” The presence of these cells in certain tumor types is associated with a survival benefit, and their relative abundance can help predict how a patient will respond to treatment. “IHC can also be used to identify proliferating cells (e.g. by detecting a classic cell proliferation marker like Ki67), an approach that can aid in determining the histopathological grade of a tumor.”
Frozen or FFPE tissue?
Understanding the difference between frozen and FFPE tissue is an important first step toward IHC staining success. Anyone who has spent time in technical support will be familiar with the complaint that an antibody validated for IHC with frozen samples is unable to recognize its target when used to probe FFPE material. “Frozen samples are often used when IHC analysis must be performed during a surgical procedure, for example to determine cancer margins,” explains David Schwartz, CSO at Cell IDx. “Compared to FFPE, the turnaround time is faster, yet staining quality can suffer as a result.”
Chandra Mohan, Ph.D., biology technical marketing at MilliporeSigma, notes that one reason for reduced staining quality is that frozen sections are generally thicker, which can impact microscopic resolution. “Additionally, the formation of ice crystals in frozen tissue samples can alter tissue morphology,” he says. “However, frozen samples have an advantage if there is a need to preserve enzyme or antigen function and should be used in cases where there is a risk of immunoreactivity being lost due to fixation.”
Zhang notes that a major benefit of FFPE tissues is that they can easily be stored long-term. “This is especially valuable in diagnostic testing where sample archiving is usually required,” he says. FFPE tissues also have excellent tissue morphology that can be more easily visualized, not least because solid fixation allows thinner sectioning.
More steps, more chance of error?
IHC staining protocols are widely recognized for being labor-intensive. FFPE IHC in particular involves several unique steps—deparaffinization, rehydration, and antigen retrieval—that inevitably extend research workflows and increase the number of places where things can go wrong. “The antigen retrieval step is often one of the most problematic,” says Mohan. “Poor antigen retrieval can lead to false negative or false positive staining and may also result in antigen loss, for example by causing tissues to become detached from the slides. Other challenging steps (common to both frozen and FFPE IHC) include non-specific antibody binding to the tissue, antigen expression below the limit of detection, and the presence of endogenous peroxidases or species with avidity for avidin-biotin complexes.”
Despite these pitfalls, errors can be reduced significantly. “Antibody quality continues to improve and advanced detection reagents are readily available to increase signal strength while reducing background noise,” comments Pohl. “Brighter, contrast-rich, stable chromogens have also enhanced results and broadened the application range of IHC. Moreover, with many steps in the IHC workflow being repetitious or very similar in nature, the amount of equipment available to improve reproducibility or even fully automate the process is likely unrivalled for IHC.” Zhang adds that modern innovations such as auto-stainers and auto-scanners have also dramatically increased throughput, as well as enabled data digitalization.
Multiplexing provides deeper insights
Although originally designed to detect a single biomarker using a simple chromogenic brown stain, IHC has evolved to allow multiplexing. This can be achieved chromogenically, for example by using Enzo Life Sciences’ MULTIVIEW® PLUS products that provide simultaneous detection of two biomarkers on one tissue section (up to four colors with a sequential staining protocol), or using fluorescent detection. “The advent of multiplex fluorescence-based tissue staining technologies enabled detection of subsets of cells identifiable only by combinations of specific markers and the relative spatial localization of those subsets within the context of the tissue,” reports Schwartz. “However, while many high-plex fluorescent technologies generate high-content data, this often comes at the expense of throughput and difficulty dealing with limited tissue samples. In contrast, Cell IDx’ UltraPlex hapten technology allows rapid, scalable chromogenic or fluorescent multiplexed IHC detection with just a single antigen retrieval step and overcomes the need to ensure primary antibodies are raised in different host species.”
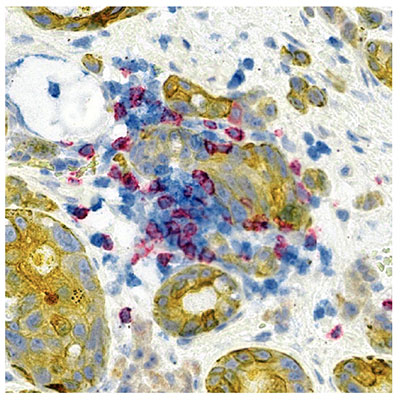
Image. Lung Adenocarcinoma stained with UltraPlex chromogenic multiplex IHC: CD8 (red), PD-L1 (Blue), Pan-CK (Yellow), 20X magnification. Image provided by Cell IDx.
IHC staining best practices
For IHC staining to go according to plan, it is important to follow best practices. The following tips combine the expertise of all four contributors to this editorial:
- Choose a tissue preparation method, frozen or FFPE, that is compatible with your downstream workflow (e.g. available cold storage facilities, need to archive samples for future studies)
- Dissect tissues into a proper size and freeze or fix them immediately upon collection to prevent antigens from degrading or translocating
- When fixing tissues, optimize the timing; this should be long enough to allow the fixative to permeate into the tissue but not so long that epitopes are permanently masked
- Avoid freezing artefacts in frozen tissue sections by employing paraformaldehyde (PFA) perfusion fixation methods followed by cryopreservation in sucrose solution (prior to OCT embedding); this method may not be suitable where antigen function must be preserved
- Consider whether antigen retrieval is required—for FFPE tissues, antigen retrieval is necessary in most cases; while the chosen method should be specific to the target and primary antibody, heat-induced epitope retrieval (HIER) in Tris-EDTA pH 9.0 usually works in the majority of cases
- Where antigen retrieval is necessary, consider using staining technologies that utilize a single antigen retrieval step (e.g. UltraPlex) to avoid possible loss/detachment of tissue and differential effects on antigen expression of multiple rounds of antigen retrieval
- Research the expected staining pattern for your target(s) of interest; keep in mind that this might be changed under certain circumstances (e.g. hypoxia, chemical treatment, or mutations)
- Remember to optimize blocking and permeabilization procedures to increase signal strength and reduce background
- Check that antibodies are validated for your chosen tissue (frozen/FFPE as well as host species); refer to the antibody manufacturer’s recommended IHC staining protocol
- Shorten protocols by using directly conjugated primary antibodies; remember that low abundance proteins can be hard to detect with directly-conjugated primaries—an HRP polymer can be helpful to enhance the signal
- Always include relevant controls; set negative controls by replacing primary antibodies with dilution buffer only to avoid false positive results—this is vital when working with blood-rich specimens
- Choose an appropriate counterstain for your tissue and application to maximize the morphological information
- Select your detection system wisely to ensure sensitivity, flexibility, and reduced background; modern detection systems have come a long way since peroxidase anti-peroxidase (PAP) or avidin-biotin complex (ABC) methods
- Mount slides with care; use an appropriate cover medium for longevity of IHC staining
- Consider using novel tools and technologies to streamline IHC protocols; combine newer systems with high-throughput autostainers and brightfield scanners/microscopes for even greater efficiencies
- Refer to manufacturers’ troubleshooting guides for solutions to common problems