Cancer immunotherapy—the effort to boost a patient's immune system, allowing it to better fight cancer cells on its own—has shown great promise for some previously intractable cancers. Yet immunotherapy doesn't work for everyone, for reasons that aren't always clear. While most research and new therapies in this field have been focused on CD8+ T cells and their binding partner, MHC-I, research published yesterday suggests that CD4+ T cells and their binding partner, MHC-II, may have even more influence on emerging tumors.
"The more we know about the ability of a person's immune system to clear cancer cells before they take hold, and the more we can combine that with other information about their inherited risk factors or environmental exposures, the better we may get at predicting a person's cancer susceptibility," says senior author Hannah Carter, Ph.D., an assistant professor at UC San Diego School of Medicine.
The Major Histocompatibility Complex (MHC) is a family of molecules displayed on the surface of most cells in the body. MHCs hold out antigens—bits of just about everything from inside cells—and display them to T cells. T cells ignore MHC molecules with "self" antigens but kill the ones with foreign or mutated antigens. While MHC-I is displayed on the surface of every cell, MHC-II is only displayed by professional immune cells, such as macrophages. Also, MHC-II is more complex and binds a larger range of antigens.
Carter’s team applied computational biology methods to data available from The Cancer Genome Atlas, the NIH’s database of genomic information from thousands of different human tumors. They scored 5,942 patient tumors based on the ability of their MHC-II molecules to present 1,018 cancer antigens for inspection by their CD4+ T cells and found that an antigen that is well recognized by MHC-II is less likely to show up in a tumor than a mutation overlooked by MHC-II. This is even truer for MHC-II than Carter’s previous study showed for MHC-I. However, Carter and team were surprised to find that, unlike MHC-I, MHC-II's ability to recognize antigens had no correlation with age of diagnosis.
As the field advances, Carter hopes researchers and clinicians will take both MHC-I and MHC-II data into account when developing and personalizing cancer immunotherapies.
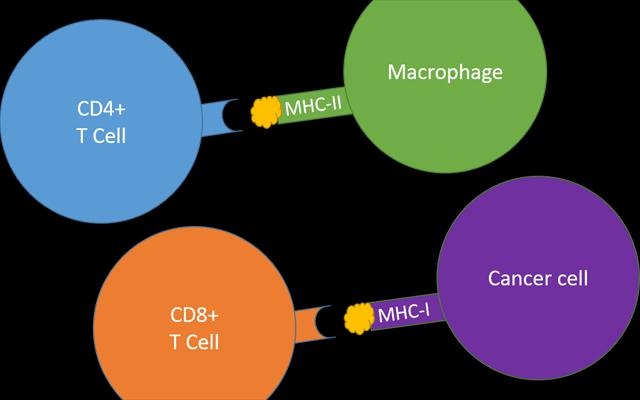
Image: Major Histocompatibility Complex (MHC) molecules display antigens to T cells, immune cells that constantly check for infected or damaged cells. If T cells spot MHC molecules with foreign antigens or mutated self-antigens (such as cancer antigens), they kill the cell before the damage spreads. MHC-II is only displayed by professional immune cells, such as macrophages, and is recognized by CD4+ T cells. MHC-I is displayed on the surface of every cell, and thus any cell with the potential to become cancerous, and is recognized by CD8+ T cells. Image courtesy of UC San Diego Health.